Paper submitted on September 2003
Posturology of the ophthalmologist
Second part
The proprioceptive system
For better understanding it
Dr. Gabriel ÉLIE
How do you feel?
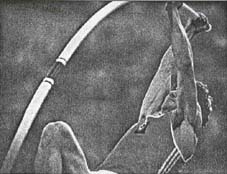
One can wonder whether the conscience that we have of our own person is not provided to us above all by this feeling, emanating from all our muscles coming to indicate to us how our arms are placed, our legs, in short in which posture is our body (fig.1). Before thinking, acting, writing, Descartes could have said, "I feel, therefore I am" (Genius of the intellectual who burn the first stage for better striking).
Fig.1- Thanks to the proprioceptive sense, the athlete knows the position of each segment of his body.
This presence of our body is provided to us by our various senses. But the sight, hearing, the sense of smell and even the taste indicate to us especially how is space around us. It is the same partly for tact. The touch is at the border. It emphasizes the interface between this extracorporal space and our own body. On the level of the skin, on the surface exist microsensors of pressure, pain. A little deeper the thermal sensors. Then, to the more inside of our body, it is the expansion of myriads of probes which indicate to us the position of the various segments of our body and their respective movements.
How are you?
At any moment, before any action, we must evaluate our position, our posture; And, at once after the gesture, to note the result of the ordered movement: Perpetual continuation of controls which allow the muscular follow-up and the adjustment of the gesture. It is this internal sense system which we call proprioception or better "proprioceptive system".
It then ties a relation between data collected by the other senses and those given by this internal tactile system to evaluate the real position of our body with respect to our environment. Among the four other senses, obviously the relation and confrontations of data are more marked with the sight. Useless to say that the position of the images (surrounding objects) on the retina and the direction of the glance are of primary importance in the evaluation of what surrounds us. And the location of what we see compared to our body makes by an appreciation of the position of our eyes in the orbits, i.e. by the extrinsic oculomotor muscles.
How do you see yourselves?
The answer is not it: "By my proprioceptive system"!. Similarity between the sight and this system (true internal vision): It is not astonishing then that these oculomotor muscles have a place privileged in the proprioceptive system and that they can intervene in a disordered state, but also in a rescue of many deficits of the postural system.
That is why Pr. Martins Da Cunha, specialist in functional rehabilitation and Dr. Alves da Silva, ophthalmologist, confronted their two specialities in a common research. For more than 20 years, their method has grown rich and stripped. It is especially with this one, that of the Lisbon School, that we will make reference in the pages which will follow.
Several hundreds of probes per gram of muscle
When all is well, we have only one very vague feeling of our internal organs. We do not feel either the usual beats of our heart. Hardly we have the concept of our breathing. But we are aware of the position of our members. How is this sensitivity organized distributed in the depth of our body, from the "eyes of the head" to the sole of the feet? The receivers of Golgi located at the level of the tendons, the palissades of Dogiel indicate to us contracture of a muscle. As Sherrington and Herring said, its antagonistic muscle relaxes. Its stretching excites sensors, the neuro-muscular spindles of an extreme complexity, located within the groups of muscle fibres. The setting in tension of these sensitive formations is a little comparable with that of a slackened elastic cord which starts to vibrate when it abruptly is stretched (fig.2).
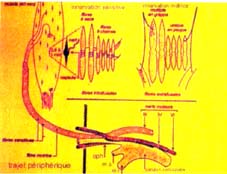
Fig.2- Diagram of the muscular sensors (according to C Battini).
And precisely these formations are also excited by applying a mechanical vibrator to the muscle. It is around 70 vibrations/sec (70 hertz) that one obtains the best effect (fig.3). Thus excited, the muscles of the calf give, for example, the impression of extension of the leg whereas this one does not move. This property allowed the team of J.P. and R. Roll, A. Kavounoudias to carry out an interesting experimentation on various proprioceptive phenomena, whose applications are addressed to the spationauts in weightlessness.
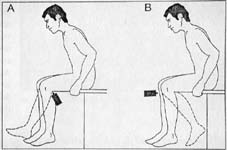
Fig.3- Vibrations applied to certain muscles give to the subject the feeling of movement, whereas his member does not move
What for is it used?
These feelings walk on by various ways to the brain. Those which would be interested by the way of the related ways and the cerebral centers will find a description of it in an excellent article of Pierre-Vital Bérard published in Coup d’œil n° 48 of 1994, from which we got the diagrams attached (fig.4). The brain perceives these impulses, analyses them and constitutes a data basis to control, coordinate, order gesture and muscular tone. Attention, if the data of the sensors are contradictory! The cerebral integration will be disturbed. The disorder which results from that can generate inhibitions affecting body balance, but exceeding also sometimes the limits of this only function. We will evoke that later.
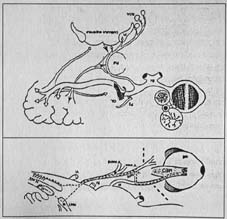
Fig.4- Diagram of the optical pathways (according to F Vital-Durand).
The proprioceptive sensors are distributed from top to bottom in our body. And certain stages are more important and perhaps more innervated. The extrinsic ocular muscles represent a privileged zone, as we said. It governs the glance. Just below, the neck muscles are significant too. The head rests as on a kneecap: it can turn to the right or the left, incline, flex or extend. It contributes to put orbits in the direction of the goal to look at. And this gesture will be refined then by the intra-orbital musculature.
Then all the other muscles of the body intervene, without forgetting the spinal ones. Ankle is still a significant relay. All these stages are in interaction, work together by summation of the data and coordination in the results. It seems, indeed, that the stage eye-neck acts for the orientation of the body in its extracorporal space and that ankles intervene in the regulation of this orientation.
And it is the foot
The plantar zone acts a little differently. Its cutaneous sensors react especially to the pressure, they are mechano-receptors. Pressures are not regularly distributed on all the plantar sole. And any movement of the body has them vary.
Curiously, the mechanical vibrations activate these sensors in the same way as for the muscular sensors. It is thus possible to have the muscular tone vary and to induce postural displacements by applying these vibrations to one or the other part of the sole of the foot. This plantar sensitivity decreases with the age. Its diminution appears correlated with the frequency of falls of ageing people. These plantar sensors also seem sensitive to the infra-reds rays sent by the heat of the foot and reflected by a sole-mirror.
These multiple stages govern the muscular tone of all our body. The data of the proprioceptive system contribute thus to our vertical balance and must be in agreement with the data coming from the semicircular canals. This feeling of balance in connection with the action of gravity is distributed in all the body. A point is particularly ready to evaluate it, they are the mandibula muscles. The lower maxilla behaves like a beam. And one saw imbalances occurring following installation of dental prostheses!
Unstable balance
A body is in steady balance when its centre of gravity is located below its base of support. It is not the case of our body located in unstable balance, since it must always fight to keep its centre of gravity above its base (fig.5), i.e. the polygon delimited by the surface of the two feet. It is to fight against the fall that the proprioceptive impulses and the muscular tone are perpetually in awakening, in order to restore balance. Continuously small oscillations vary the line of support of the centre of gravity, perpendicular on the ground. This one described a surface does much smaller than that of it corresponding to the sole of the feet (fig.6).
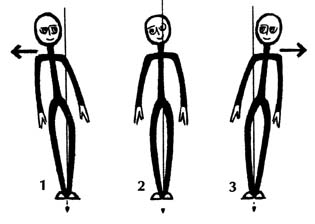
FIG.5 — If the centre of gravity of the body goes out of the support basis, balance is worn-out.
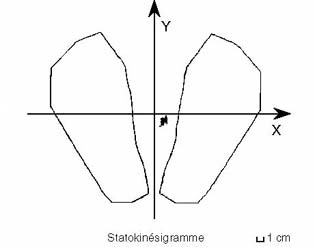
FIG.6-Statokinesigram: Normally, the oscillations of the perpendicular on the ground gone down from the centre of gravity of the body remain in a small surface, in the center of support basis. In case of deficit, this surface gets bigger sharply
As soon as there is a disorder of balance, this surface of oscillations widens. If it exceeds the plantar basis of support, corrections have to be made otherwise the subject falls. Some subjects may have a resting support more on one foot that on the other. One speaks about plantar support right or left, often with an unequal division between the two. We will give more explanations latter. But a unilaterally exaggerated tonicity can cause contractures, source of tiredness, cramp, pain and of a multitude of other disadvantages.
|
Sorry… I am lazy… But I spent to much time correcting the automatic translation for those who do not know how to speak French… From now on it is no longer corrected !…
|
Posturology of the ophthalmologist
Third part
The Syndrome of Postural Deficiency
of Martins da Cunha in clinical practise
Dr. Gabriel ÉLIE
In the preceding article, we tried to summarize the proprioceptive system, so useful for the conscience of ourselves. But there are sometimes deficiencies of this "sixth sense". And the ophthalmologist is often brought to note them. He can also look after them. We will see it in a later article.
Subjective multifacettes of postural deficiency
We are for the majority in asymmetry: Result of our constitution, our practices, our way of life. But we compensate for this unilateral prevalence and we do not have disorders. It is not the same for others. Indeed, each one has a variable resistor. This personal resistance can also be put in failure if it is confronted with varied tiredness or other circumstances: living conditions, work, traumatisms, etc…
Postural deficiency results then in a large variety of functional disorders. Despite everything, some are more frequent. We thus will enumerate them, without having the claim of all to name them. They can occur at any age and they are soignables at any age.
Disorders of the muscular system
: Permanent tiredness. Difficulty of making certain articular movements or of the members, hyperalgie of the shoulder. Retrognatism mandibulaire, spasm of the ptérygoïdiens. Muscular pains. Stiff neck, cervicalgie, rachialgie, sciatalgie, lumbar pain or inguinale, thoracic or abdominal pain without organic lesion simulating a medical urgency. Dyspareunies. Buzzes of ear. Pareses, paraesthesias.
Disorders of the system vasomotor:
Paleness of the skin, Syndrome of Raynaud (fig.7), pinching enters the maximum and minimum blood pressure, cephalgias, migraines.

Fig.7- Syndrome of Raynaud: temporary vasoconstriction of digital circulation.
Disorders of somatognosis and the space orientation:
Inaccuracy of the movements, dysmetry, bite of the language or the interior of the cheek. Unexplainable falls, distorsions with repetition. Disorders of automobile control. Deficiency of ocular convergence, exotropie of near, instability of the amétropie.
Disorders of psychism:
Agoraphobia. Strategy of hyper or hypoactivity. Tired alarm clocks. Deficit of the concentration. Depression with an accompaniment of other proprioceptive signs, but resistant to the treatments medicamentous and disappearing with the postural reprogramming.
Disorders of perception:
Deformation of the visual image, monocular diplopia, scotomisation. Deficit of auditive perception: These people listen without including/understanding. Dyslexia.
Disorders of balance:
Infirmity with walk, giddinesses, imbalance.
Disorders of the system vagal:
Nauseas, vomiting, cold sudation of the members.
Dyslexia
In the children, the more frequent disorders are the dyslexia (see the article companion), dysgraphia, dysorthography, the deficit of training, the loss of concentration, the frequent épigastralgies, falls, shock against the objects. The deafness of perception.
dyslexiaIn front of this significant number of demonstrations of a postural deficit, one would quickly come from there to think that many complaints of patients can come from there. One would especially not have to be mistaken there. It is necessary to have the obsession of another organic cause. A proprioceptive cause should be evoked only when very other causes was drawn aside by the suitable examinations.
The single facet objectifies postural deficiency
dyslexiaOne of the characters of the syndrome of postural deficiency (SDP) is that the complementary examinations, imagery of all kinds, test of Barany, analyses biological prove to be negative. The treatments of test with anti-inflammatory drugs, tranquillizing, soporific bring only little or nothing. Once the eliminated organic cause, one can think of a functional origin of deficiency of the proprioception.
The clinical examination then will show a remarkable similarity in the objective signs observed. And this, in spite of the large variety of the functional translations described above.
In fact, almost all the clinical signs that we will observe highlight the bad postural interpretation of the brain. This one causes one cramp generalized with unilateral prevalence.
A body of flesh or stone?
- Appreciation of the position of the feet:
The subject should not look at its feet. Upright, the right glance in front of him, one positions his left foot good right parallel with the antéro-posterior axis of its body (fig.8) the right foot is then slightly put in back withdrawal, but he as well parallel. One asks then about saying how it evaluates the position of its feet. Parallels: the appreciation is good. In convergence:, the appreciation is erroneous. For better knowing his answer, one asks him to position his hands for mimer the position of his feet. The disorder of appreciation is obvious. One points out it to him.

FIG. 8 Without looking at, the subject simulates with the hands the supposed position of its feet. In spite of the parallelism of the feet, it thinks that they are in convergence in the event of SDP.
- Limitation of tonic convergence:
One asks about fixing the point of a ball point pen by just bringing closer it at the height his eyes. The pen must be presented oblique and nonvertical or horizontal, in the axis of the face, Déjà, towards 30 to 25 centimetres, it tends to flee while carrying its head behind. It has the feeling to converge too much. Or, one of its eyes takes down, but without leaving in divergence (with the difference of what occurs in the insufficiency from usual convergence).
- Test hand-eye
The dominant hand flat the palm downwards, fingers wide coupled except the inch drawn aside to the maximum. One traces with the ballpoint pen a line connecting the bottom of the cavity between the métacarpiens and the arc of the cutaneous support connecting the inch and the index. This mark is thus perpendicular to the concavity of this support (fig.9).


FIG. 9 Test eye-hand:
By a movement in mowing, the reference mark between inch and index must be superimposed on the object concerned (photo of left). In the event of deficiency, the impact shifts towards the index (photo of right-hand side), bad aiming of the object-target.
One then presents the vertical pen at a distance a little less than the length of the arm. By a rapid horizontal movement of mowing, one asks about putting in coincidence milks it his hand with the pen. In the event of deficit, the pen runs up against the base of the index, i.e. 1 or 2 cm of the reference mark: bad appreciation of space. One points out it on the subject.
- Opening of the mouth:
The subject can return in its mouth 2 to 3 fingers, the horizontal hand in a sagittal plan (fig.10). One marks on his fingers by a feature of pen until where it can return them. This test will be used as comparison to evaluate the result after treatment which should relax the muscles masticateurs (fig.11). The same applies to the rise in the arms to the vertical. It will be facilitated after treatment.

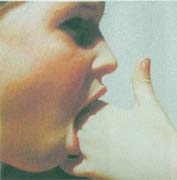
Fig.10- Contraction of the muscles masticateurs: The 3 fingers penetrate only of approximately 2 phalanges. To mark the penetration by a feature of ink on the index. Fig.11- From the very start of the treatment, the mouth opens larger, the fingers penetrate more amply: the feature of ink is largely exceeded
- Rotation of the head:
The quite right head neither leaning on the side, nor in deflection, one requires about turning the head in rotation of the neck towards the right shoulder (fig.12). One measures the distance between the acromion and the medium of the chin. Even operation made in rotation towards the left shoulder (fig.13). One estimates towards which side the head can the least turn (fig.14). The subject often smells itself that it is limited more on a side and that its sternocleidomastoid muscle is more contracted side of this limitation.
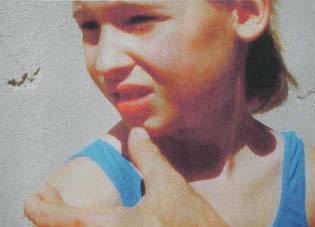

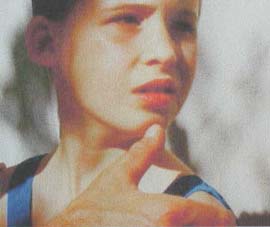

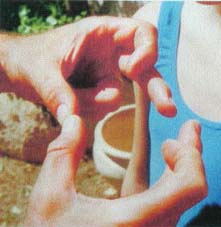
Fig.12- Rotation of the head towards the right. The distance acromion-chin is measured Fig.13- Rotation of the head towards the left. Measure distance acromion-chin. Fig.14- Comparison of these two distances. The contraction of sternocleidomastoid attaches the rotation of the head
- Deflection of the head behind
: One makes slip from top to bottom on each side of the neck his hands until they stop on the side muscles binding the neck to the shoulder. Then one asks about letting leave his head behind. One then appreciates the height between the side of the index of the inspector and the ear of the subject (fig.15). Usually there is correlation between the side where this distance is less and the side or the head goes less further in rotation.
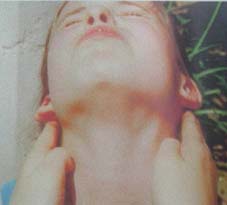
FIG.15 - Deflection of the head. Quite visible asymmetry: the ear touches the side of the index on the right, not on the left.
A research with the range of all ophtalmo
In the event of SDP, one will find an anomaly with each one of these tests, whatever the disorder about which the patient complains.
The examination stops there in the majority of the cases. It took a few minutes: No complicated instrument, only one clinical study for which it is necessary to be initiated. As usual in an ophthalmologist, the subject remains equipped.
Admittedly, it would be wise to better know the plantar support. But the fact that the subject feels épié modifies its attitude; and the experiment showed that one can with difficulty proud with the results of this study. We will make use of it nevertheless, a little later, to mean the various postures of balance. But the Portuguese clinical examination does not employ a stabilometric platform and is not useful itself either of the test of trampling of Fukuda. It is the great difference between the Portuguese school and the French school.
Posturology of the ophthalmologist
Fourth part
Treatment of Syndrome of Postural Deficiency
Dr. Gabriel ÉLIE
In the preceding articles, we wanted to draw the attention to the postural deficits. We came from there now to the treatment
Unicity of the treatment
Prisms, soles; postural rehabilitation. The treatment does not vary or if little, whatever the disorder. The clinical experiment is there to reinforce this policy. But these three pillars form a unit which one should not dissociate with the risk not to have a result. Let us detail it.
- prisms
It is in their regulation that there are some alternatives:
In the majority of the cases, we find a coherence between the side where the rotation of the head is limited and the side of the least distance between the blank of the hand of the inspector and the house of the ear of the subject (see preceding article). It is the case by far most frequent, that is to say 90% of the subjects. It is necessary to give an oblique prism on each eye, so as to slacken the 2 oblique small muscles. The base of the prism is thus turned into supéro-temporal, with 125° on the right and 55° on the left. The power of the prism is 2 dioptres for an eye and 3 to 4 dioptres for the other (never more). The strongest prism is put side where the rotation of the head is limited.
This case of good correspondence between the 2 movement-tests of rotation and deflection of the head always corresponds in a pure mixed plantar support (cf case "E" of the synoptic table); i.e. an almost equal distribution of the support on the 2 feet. Usually these 2 feet rest on the ground in divergence, i.e. that the heels are brought closer than the points and about on the same level of before behind. But we repeat that this plantar classification does not have a great importance for the Portuguese school.
The lion in the cage:
When there is no correspondence between the 2 tests of rotation and deflection of the head, it is necessary to specify the regulation of the prism by an orthoptic examination with the synoptophore of Clement Clarke. With this instrument and him only. It is the test of the directional scotome. The head of the subject should not be tilted forwards or backwards, quite right if possible in its usual position, fixed on the mentonnière. On the other hand, it would be preferable to remove the frontal support of the instrument which can induce unusual positions of the head.
One makes the development of the pupillary variation. One seeks the angle where it is easiest for the subject to see the lion and the cage well to superimpose itself. It is with 0° or near and the two arms of the synoptophore are solidarized. And one turns the axis of the synoptophore of 20° in the glance towards the line (dextrogyre) (fig.16 and 17), then in the glance towards the left (fig.18) (laevogyrous).
 |
 |
 |
| Fig.16- Seeks directional scotome: The synoptophore turned towards the line | Fig.17- Seen in overhang of the rotation of the synoptophore and the glance towards the line | . Fig.18- Seen in overhang of the synoptophore and the glance towards the left |
The selected images are the large lion and the cage (test cards G 3 and G 4 of Clarke: lion in front of OD, cage in front of OG (fig.19). But the phenomenon also occurs with the small lion and the small cage of the same test of the macular series). The test must be done in attenuated light One will notice that as the eyepieces of the synoptophore are turned, certain bars of the cage or certain parts of the lion disappear, indifferently on the test positioned on the right or on the left (fig.20 and 21). Disconcerting and curious test: This eclipse of part of the one of the tests is fugitive and it is necessary to be prevented of it to notice it. It could pass unperceived. It is indeed a cerebral phenomenon of inhibition limited, difficult to explain. The school of Lisbon makes use of it in an interesting way as we will see it. With him only, this test justifies the title which we would like to give to all these chapters: Posturology of the ophthalmologist.
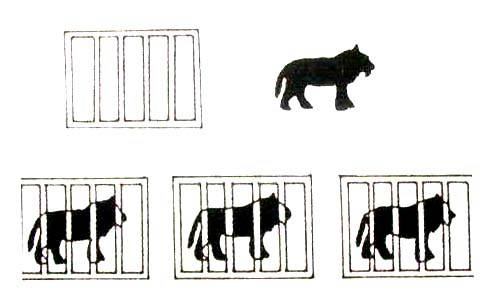
Fig.19- Tests employed for the research of the directional scotome: the lion and the cage

Fig.20- In this case, the scotome occurs in the glance on the left: Some bars of the cage miss, whereas, in the right glance in front of oneself or on the line, the lion and the cage are entirely seen.

Fig.21- Even phenomenon, but in this case lion and cage are cut down. The significance is identical to that of the preceding case
Lucky find of the ophtalmos for the 10% remainders
4 cases should be distinguished then:
- the directional scotome occurs in the glance towards the left towards 20°. No the scotome towards the line. One must put a prism on the right eye bases temporal, horizontal axis. This corresponds in a plantar support right (cf case "has" synoptic table).
- the scotome occurs in the glance towards the line towards 20°. No the scotome towards the left. One owes prismer the left eye bases temporal, horizontal axis. This corresponds in a left plantar support (cf case "B" of the synoptic table)..
- the scotome occurs in the glance on the left as of 20° and also in the glance on the right, but not before a rotation of 30°. One prescribes a prism on the right eye bases supéro-temporal centers with 125°. It is about a plantar support mixed right (cf case "C" of the synoptic table).. To go until 30° of rotation, it is necessary in certain models of Clarke to disunite the two arms of the synoptophore. If not rotation is blocked towards 25° approximately.
- the scotome occurs in the glance on the right as of the rotation of 20° of the axis of the synoptophore, but not before 30° in the glance on the left. One prescribes a prism on the left eye bases supéro-temporal, axis with 55°. It is about a left mixed plantar support (cf case "D" of the synoptic table)..
Sometimes, the scotome appears only for one more significant rotation, until 40°. The significant one is to note which is the shortest rotation, dextrogyre or laevogyrous, which causes the phenomenon; And to see whether it is plain or bilateral.
Let us notice that the prism is always put on the eye located on the side of the plantar support dominating and especially opposed to the fastest appearance of the scotome.
If one wanted to make the test for a pure mixed support, case describes into very first, the scotome appears as of a rotation of approximately 20° as much on the left than on the right. But this examination is not necessary since there is coherence between the two tests of rotation and défléchissement of the head: This coherence signs a pure mixed plantar support. As indicated above, the prismatic regulation is then bilateral with a variation of power from one eye to another. Let us recall that it is 90% of the cases.
To defer to the synoptic table, on which one will include/understand better the position of the feet according to the plantar support --
|
Case
|
Test with the synoptophore: the scotome appears
|
Position of the prism
|
Corresponds to
|
|
|
glance to the R
|
glance to the L
|
plantar support
|
||
|
a
|
No scotome
|
at 20°
|
RE 180°
|
a) Right
|
|
b
|
at 20°
|
No scotome
|
LE 0°
|
b) Left
|
|
c
|
at 30°
|
at 20°
|
RE 125°
|
c) Mixed Right
|
|
d
|
at 20°
|
at 30°
|
LE 55°
|
d) Mixed Left
|
|
e
|
at 20°
|
at 20°
|
RE 125° + LE 55°
prism most power on the side where the rotation of the head is limited |
e) Mixed Pur
|
 |
 |
 |
 |
 |
|
a) Right support
|
b) Left support
|
c) Mixed right
|
d) Mixed left
|
e) Mixed pure
|
Let us remember already that one of the feet is posed more through that the other. It is the additional foot of support. The corresponding leg and the thigh have a hypertonus for their external rotatory muscles and bungee cords. The treatment aims at equalizing the muscular tone of the two legs. But not only of the leg…
What is still necessary for this prism?
We have just spoken about the position from the prisms: side, bases, axis. But which power to choose? It is in fact tiny and never exceeds more than 4 dioptres. Beyond, it causes a diplopia. The postural effect is not possible any more.
It is the immediate result on the tonicity of the muscles which will guide the choice of the power. One puts on glasses of test a prism of 2 dioptres in the child, of 3 dioptres in the adult with the orientation indicated. Or a prism on each eye, in the event of pure mixed support. We already said it.
And the tests are remade:
Appreciation of the position of the feet, tonic convergence, test eye-hand, rotation of the head and opening of the mouth. Which astonishment to see from the start the asthénopie convergence to disappear, the test eye-hand to standardize itself, the rotation of the head to equalize itself and fingers to engulf itself in a mouth more opened much by relaxation of the muscles masticateurs.
If this standardization is insufficient, it is necessary to pass to a prism of 1 higher dioptre. Usually the average power necessary is a little lower in the child in regulation plain or bilateral. The appearance of a diplopia signs that it is necessary to decrease the power of the prism unless one was mistaken in his orientation.
In the pure mixed plantar support, the most frequent case, why does one generally require for 2 dioptres on the right and 3 on the left if the subject is originating in the south and generally 3 on the right and 2 on the left for the Scandinavian origins? What of still unexplained things?
Spectacles, and good ones!
The glasses are carried out in a good optician. If the person needs a ametropic correction, it should be mixed with the postural regulation. Useless to say that the pupillary variation must be scrupulously respected, if not one is likely to generate another nonrequired prismatic effect which could distort the regulation. The stability of mounting is significant. The optician must take care to give a solid, not very deformable mounting and with good to adjust it with the face. One advises a light elbow of 3° on the level of the nose in the frontal plan (fig.27) and a slope of 15° on the vertical (the bottom of glass behind). For the children, a small plastic bridge resting on the nasal edge still reinforces stability. As soon as the glasses are developed, it is wise to put them on the turntable of a photocopier. This photocopy will make it possible to supervise a possible deformation and to indicate that a re-arrangement is necessary.
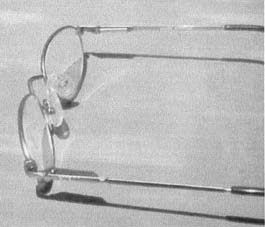
FIG. 27- the glasses must have a slope of 15° on the vertical. The plans of glasses are shifted one and the other of 3° on the level of the nose.
The regulation of prisms is an astonishing manner to correct the muscular tone and thus the postural deficit. This regulation is one of the principal keys which makes us return inside the proprioceptive system to recondition it. Its action is allowed like causing a relieving of the external rotatory muscles and bungee cords of the lower limb opposite than the prismatic eye. But it relaxes in fact the hypertonic muscles top in bottom of the body. In spite of its paramount effect, it is not with him only sufficient. To neglect the other keys of repair would be often to go towards a failure with besides of the badly supported prisms. It is now necessary to deal with the sole of the feet and the postural reprogramming.
Soles? But which kind?
If the regulation of prisms has been recommended for a few decades, it had seemed much more obvious for a long time that imbalances of the statics of the body could be compensated by a thicker sole on the right or on the left. And his effects had not been spared. After an examination of the spinal column, iliaques spines, one prescribed larga manu. But was to forget that the feelers and plantar muscles, too requested, could end up being atrophied and the result became opposite. Beyond an extra thickness of 3 mm, there is risk of crushing of these receivers, with appearance of harmful, noxious zones. These noxious zones are due also to deformations of the foot. The shoes are often also the cause.
The Portuguese school thus gave up the soles of compensation to use another system based on the reflexion of the infra-reds sent by plantar heat (fig.28). Small infra-red mirrors placed on the level of the arch of the foot encourage the toes to bend during walk at the time when the foot passes from the horizontal plantar support to the former support.
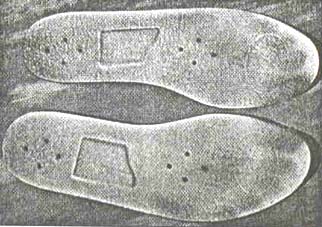
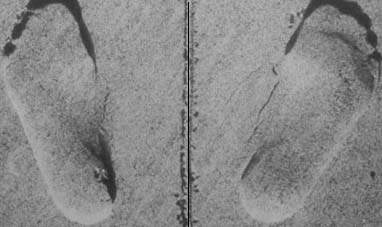
FIG.28 - postural soles: The trace of the supports is noticed on these a little worn soles. The ombrée zone corresponds to the big toe, thus stressing its dominating role the mirror reflecting the infra-reds is at the level of the arch of the foot.
The big toe is one of the keys of our balance. This incentive with the work of the toes acts on the muscular tone of all the lower half of the body. It was studied by stereophotogrammetry. This method consists in sending parallel beams of shade and light in successive, tangent layers with the dorsal muscular relief. It emphasizes the changes of this relief. One can thus determine that the prisms would act especially on the higher part of the body while being reduced out of V to finish to the bottom of the spinal column (fig.29). On the other hand, the plantar impulses act on the bottom of the body on a zone in the form of M, whose higher concavity would frame the bottom of V.

FIG.29 - the prisms act on the higher part of the body until the bottom of the spinal column. The soles influence the lower part by framing V superior.
The sole in the sock
If it is wanted that the soles act, and that the reflexion of the infra-reds is not lost, they should be carried to same the plantar skin. Not to hesitate to introduce them into the socks.
One cleans them with a cotton soaked with alcohol. They are washable also with the washing machine, but never at a temperature of more than 40°. If they were to be shortened a little, it is necessary to measure the shortening necessary, then, to remove a third of measurement to the heel and two thirds with the point. So that they find their place, it is often necessary to add a size moreover to the shoes, especially for the children.
The soles are always the same ones. Only the size changes. One can order them with the following address:
Soles INFRA
Mr. J Rodrigues, Apartado 598, 2685-601 Portela LRS Portugal
Such: 00 351 2 19 43 16 72. It speaks French.
Postural rehabilitation
Once the prescribed glasses, the bought soles, the subject is provided with its principal material. Soon, it is accustomed to the port and the some visual modifications that that involves. It finds the other people smaller. And that, in the absence of diplopia. With the proviso of answering the postural deficit well, these prisms are extremely well supported. On the other hand, the "prisms of reduction" included in certain progressive glasses are it much less. They were included to make glasses finer in their higher part and to facilitate downwards the glance in vision proximale. Many intolerances to progressive would be due to these prisms. It would be often wise to ask that they are removed, which can make the manufacturers (Essilor, Rodenstock).
The subject will have to provide itself of more than perseverance for its postural rehabilitation.
Rehabilitation in four dimensions: Upright and walk, sleep, breathes, read and write.
- Upright and walk
Upright, for the stop, it is necessary to supervise its position upwards. The feet are put parallel, the foot right slightly in withdrawal. The body a little ahead must rest rather on the left leg. To return the belly and to advance the shoulders a little. The hands meet ahead. The right head, the slightly sunken chin. If you want a model, look at the wife of Ramsès II, the queen Néphertari (fig.30), or go in Abou Simbel.
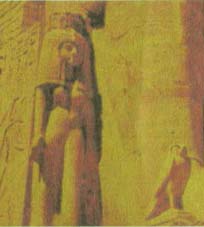
FIG.30 - Nephertari: posture upright optimum
Supported against a wall, to put the 2 feet with approximately 5 to 10 cm in front of the wall, the legs stiff. The remainder of the body as indicated above. The back stuck enough to the wall (fig.31).

FIG.31 - Attitude leaned with a wall: The quite parallel feet are isolated wall of approximately 10 cm. The dorsal curve is rectified. The head is in light inflection. The incisors are touched by their edges. The hands are cross ahead. In this attitude, one supports ventral breathing.
During walk, to advance the quite parallel feet (fig.32), not of duck walk (fig.33). The foot must roll on the ground of back ahead in 3 times: pose heel, plantar plate, then toes. The soles refléchissantes must be able to help this movement. But it is necessary especially that the shoes are not concerned ahead out of spatula ski (fig.34). If not, the toes cannot do their work. The sole of the shoe should not be too elastic. The foot must feel the ground.
The children relearn to walk rather quickly. For the adults, it is necessary that they think of it longer before acquiring it spontaneously.


FIG.32 - Walk quite parallel feet. To recommend. FIG.33 - duck Walk. To proscribe FIG.34 - to remove: the shoes of which before rebic
- Sleep
It is necessary to sleep on a quite horizontal mattress and rather hard Éventuellement, a sheet of plywood with a light flexible pavement of 5 cm is enough. The pillow passes from the bedside to the bottom of the bed. Its function is to raise cloths to leave the free feet of the weight of cloths and covers.
On this surface, 2 positions of greater relieving are to be privileged:
- On the back, well flat, the right legs and the quite vertical feet (fig.35). The pillow prevents the tendency of the feet to fall down on the sides under the weight of cloths.
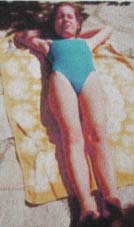
FIG.35 - Attitude of sleep: On the back, the feet quite parallel. The pillow raises cloths and not the head.
- the second position is more complex. To refer to the photograph (fig.36) for better including/understanding. On the belly, the well lengthened and brought back right leg a little ahead, the arm behind lengthened right along the body. The folded left leg makes like one 4 with the opposed leg, and its kick rests on the calf of the opposite leg. The left arm folded up, the hand well flat in front of the figure. The face is turned towards the left. In this position, the glance must see, in same alignment, the left elbow, the left knee and the end of the right foot. It any more but does not remain to be let go, slackness on the mattress. The basin and the shoulders subside.The pillow does not have any more its raison d'être under the head. One could discuss same the opposed side, but it would seem that circulation is done less by light cardiac compression…

FIG.36 - the best Attitude of sleep. It supports the muscular relaxation.
- Breathes
Two exercises are recommended during 5 minutes each one, each day. The account-minute avoids the cheating.
- the first is done upright, leaned against the wall in the position already described above. It is necessary to privilege abdominal breathing to make work the diaphragm. It is also necessary to expire gently the residual air, that which one usually leaves in his lungs at the end of the expiry. To let slip by between its incisors joined together by their edges. This position of the jaw releases the trigeminal nerve which passes close to the articulation of the lower maxilla.
- the second respiratory exercise is done lying on the back, after having put a chair laid down across the bed (fig.37). The legs must make a little Z Rentrer the belly, the back well flat. To expire well à.fond between the incisors and to inspire by preferring abdominal breathing. To help this breathing while supporting with its hands on the top of the belly.
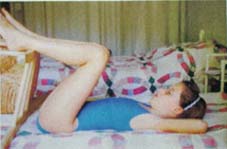
FIG.37 - respiratory Attitude of exercise: Legs in Z raised by a chair.
- Write and read
The European standard of sat of a chair is 44 cm above ground-level. Taking into account that, it should be calculated a rest-foot so that the hollow poplity takes off slightly of the plate of the chair; Of approximately 2 fingers (fig.38). For example, for the children from 8 to 9 years, the rest-foot is approximately 16 cm high. To check if the seat of work at the house or the school corresponds well to the standard. If not, to rectify the height of the rest-foot of in order to obtaining as much that the knees are slightly higher than the hips.
The book, the book is put on a desk posed on the work table so that the reading or the writing is done on a tilted level of 30° on the horizontal one. These two installations become even more useful for a dyslexic child. It is necessary to make accept these installations by the teachers. Any mom is able to build out of plywood the footrests and the desks for the class and the house. She will find the force of persuasion to also impose it on the school. With your rapporteurs, square and meter of dressmaker, Mesdames. The dads, you do not type on the fingers!And which pleasure of then seeing changing the behavior of your child.
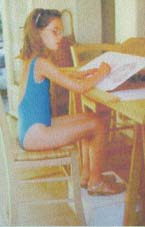
FIG.38 - Attitude of reading and writing on level inclined with 30° on the horizontal one. Feet on a rest-foot which raises the knees compared to the hips slightly. Particularly recommended for the dyslexiacs.
The follow-up, results
The glasses are to be carried as often as possible, of the rising to sleeping. However, there is a certain remanence of the effect of the prisms which can go from a few fifteen minutes at the time of the tests (attention, that is to be taken into account in the evaluation during the examination) until several days after a prolonged port.
A visit in the optician to rectify mountings is useful at the end of 6 months. Especially if the photocopy of mounting reveals a deformation. The ophthalmologist will like in the first times to re-examine his patient more quickly to appreciate the results. With more experiment, it will space controls at one year.
Of course, as far as possible, for the postural reprogramming, the assistance of an adviser makes it possible to specify certain details forgotten for walk, the station upright, the sleep. It can check if all is well implemented and to recall that it is about a whole where nothing must be abandoned.
Three effects which could pass unperceived
Progress is sometimes immediate in the field of the muscular tone. Thus some disappear quickly diminish. It is remarkable that, as soon as the prisms in place, the waist measurement decreases. The trousers do not tighten any more with the belt. Certain people have an impression of relief, of lightness. It is easier to raise the arms in the air. Attention with the dyslexic children at which this feeling of wellbeing would easily encourage not to make effort more.
When exist painful points, the installation of the prism makes them disappear almost at once. Sometimes these points are to be sought (fig.39). They are highlighted at the percussion of the cheek, the palpation of the base of the neck, the average third of the dorsal face of before arm, the grill intercostal just below and apart from the centre and, on the opposed side, on the level of the supply mains of the thigh close to the hollow inguinal. It is the same for the 3 points of Hartmann; painful points on the level of the angle supéro-intern of the orbit, the temple and the nape of the neck.

FIG.39 - various frequent painful points in the event of SDP.
This whole of measurements also seems to act on the system sympathetic nerve and parasympathetic. It follows a vasodilatation, visible sometimes with the level of the face, which recolore, even more obvious by thermography of the face.
Finally the cerebral cartography shows a standardization of the neuronal activity. Before the treatment, the cerebral cartography for the slow waves delta and téta indicates an asymmetry marked between the two hemispheres. There are zones of hypermicrovoltage. The power can go up up to 1500 to 1600 microvolt-square. After treatment, the voltage is standardized around 200 to 300 microvolt-square.
It is perhaps what explains this new aptitude for memorizing, with the training which supports progress of the dyslexic children. One can appear oneself that inhibitions, for which the child required to neutralize certain postural impulses in contradiction with others, extended beyond this function to overflow towards other cerebral functions which they inhibited too.
Of course, one is in the field of the assumptions. It was easier to find the way between muscular disorders and postural deficiency. One needed all the smoothness of the clinical observation, of which made proof Martins da Cunha and Alves da Silva to attach the dyslexia to the SDP.
But the delay that these children took obliges to restructure all that they badly assimilated. It is not the moment to slacken the efforts. "When iron is hot, at this point in time it should be modelled", likes to say Orlando Alves da Silva.
And the orthophonist?
The meetings of orthoepy for the dyslexiacs, the school exercises must continue. But the attention of the child is more constant, the comprehension of the grammatical mechanisms is done better, the memorizing of the orthography improves, the writing is standardized, the gestures become more precise. The representation of its body (standardization of the test eye-hand) enables him to better perceive where is its left and its right-hand side, where are before and back, before and afterwards. The copy and the reproduction of memory of the "complex figure of Rey" show an improvement. Progress is easier but are not acquired as by magic. The effect of the extra-curricular behavior is more quickly obtained. I return the reader to the interview of a mom of front dyslexiac already published.
When can one remove the prisms? For that, it would be necessary that the patient is able spontaneously to keep a correct posture without his prisms. It is rather rare especially in the adult.
In practice, an annual balance sheet remakes the point, modifies if necessary the regulation and takes stock of the symptoms and the objective signs. To reverify the unit as soon as the patient smells himself less better.
FIG.40 - Towards new discoveries: Lisbon at the time of caravels.
Bibliography:
ALVES DA SILVA O and Al: FUSION, Visual information and Proprioceptivity. Procedings XVII Meeting of ESA Madrid 1988 J Murube del Castillo Editor. p.89-93.
BARON J.B. Prismatic Correction in the subjective syndrômes post-commotionnels. Bull. Soc.Belge. Opht. 1963, 133,245.
BÉRARD statement: Proprioception and ocular motility. Glance 0pht.1994, n°48, p.26-39
BÉRARD statement and O ALVES DA SILVA: Postural prisms. Their in practice daily use. Opht.1994 glance, n°53 p. 29-36
Martins da Cunha H.: The syndrome of postural deficiency, its interest in ophthalmology. Day. France of ophtalmologie1986, 9, p;747-755.
GAGEY P.M.: oculomotricity as endocaptor of the postural system. Agressologie 1987, 28, p.899-903.
ROLL JP. and ROLL R.: The proprioception extraoculaire like element of postural reference and space reading of the retinal data Agressologie1987, 28, 905-911.
VITAL-DURAND F: Functional anatomy of the optical ways intracraniennes. Encycl. M-Chir. Opht. 1986, 21008 A 40,4-11-04.
Return to the banner page